Thanks to modern ART methods we today have a broad spectrum of therapy options to help you. Beginning with a mild treatment to cure minor menstrual cycle disorders to test tube (in vitro) fertilization. As soon as we have the exact diagnosis, we will find the most individual way to increase your chances of conceiving.
Hormonal monitoring/Ovulation induction
The menstrual cycle can be monitored very closely by ultrasound scans and hormone assays. With help of these very individual findings we can predict the optimal time to conceive. In many cases this method alone will result in a pregnancy. If a woman is suffering from anovulation, the maturation of the oocyte as well as ovulation can be induced by an injection of a particular hormone, which increases the chance of a normal fecundation.
Intrauterine Insemination
Intrauterine insemination (IUI) also is a procedure for treating infertility. Sperm that have been washed and concentrated are placed directly in the uterus after ovulation induction. This can be done in a natural cycle after monitoring or, to higher the chances, after mild hormonal stimulation. This treatment is easy to perform without any pain for the patient.
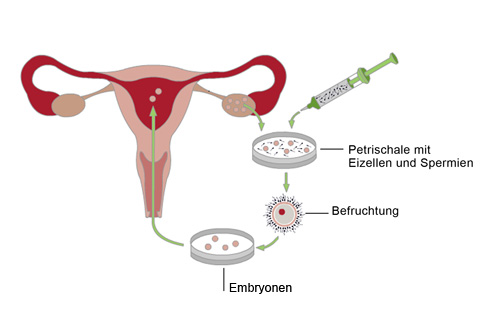
IVF and ICSI (Intracytoplasmic sperm injection = inject sperm into egg)
IVF and ICSI are also called artificial insemination (formerly test tube fertilization). The oocyte is fertilized outside of the woman’s body. To be successful, it is helpful, to induce the maturation of more than one egg. This is done by hormone injections to stimulate the growth of multiple follicles. Stimulation usually starts with the beginning of the cycle with daily hormone injections. After about 14 days the oocytes are retrieved by ultrasound guided follicle aspiration (A needle is passed through the top of the vagina to get to the ovary and follicles). Then sperm and oocytes are put together in the lab (in vitro: about 50 000 motile sperm/oocyte approx. 4 hours after retrieval) or ICSI is performed.
The ICSI is performed under a special microscope with a 400x magnification. An individual sperm is selected by the embryologist and sucked into a very thin needle and with help of specialized micromanipulation tools is injected directly into the oocyte.
Nach der Eizellentnahme wird die Einnistungsphase des Embryos hormonell unterstützt. Hierzu werden Hormonkapseln in die Scheide eingeführt. Zwei Wochen nach der Eizellentnahme kann mit einer Blutuntersuchung festgestellt werden, ob eine Schwangerschaft eingetreten ist.
The next day fertilization can be observed to a percentage of 65 – 85% of all mature oocytes. 3 to 5 days after oocyte retrieval 1 to 3 embryos (The German embryo protection law allows the transfer of a maximum of 3 embryos) are transferred into the uterine cavity with abdominal ultrasound guidance.
Nidation is supported with additional hormones, which are inserted into the vagina (luteal phase support). Two weeks after embryo transfer we do a blood test to find out, if the patient is pregnant.
IVF and ICSI will be our treatment option, if the fallopian tubes are blocked or damaged (IVF) or, when the sperm quality is reduced.
TESE
TESE – Testicular Sperm Extraction (involves a small incision and snipping off some tissue from inside the testicle – done at our clinic by an experienced urologist) is necessary, when there are no spermatozoa present in the ejaculate. If spermatozoa can be found in the testicular tissue, the tissue is frozen and thus preserved to be used for an ICSI.
Kryotransfer
Transfer von befruchteten Eizellen aus einem früheren IVF/ ICSI Zyklus
TESE – Testicular Sperm Extraction (involves a small incision and snipping off some tissue from inside the testicle – done at our clinic by an experienced urologist) is necessary, when there are no spermatozoa present in the ejaculate. If spermatozoa can be found in the testicular tissue, the tissue is frozen and thus preserved to be used for an ICSI.
Frozen embryo transfer
Surplus fertilized oocytes (spare 2PN), which can’t be used for the transfer in a fresh cycle, can be preserved for future transfers by two methods, which both routinely and with great success rates applied in our clinic. They are called vitrification (ultrafast freezing) and slow freezing. For frozen embryo transfer the patient’s endometrium is prepared for implantation usually by mild hormonal stimulation given orally. In some cases the transfer can be done during the natural cycle and sometimes a few hormonal injections are required.
Cryopreservation of tissue
Testicular tissue as well as ovarian cortical tissue and spermatozoa can be cryopreserved. There are multiple reasons for undertaking these measures. Cryopreservation of spermatozoa for example can be necessary, if the partner can’t be present at the clinic the day of the intrauterine sperm injection (IUI) or oocyte retrieval.
Blastocyst culture
By blastocyst or prolonged culture the embryos intended for transfer are cultivated for 4 to 5 days in the lab. The decision, which fertilized eggs are going to be selected for transfer has to be made till 24 hours after oocyte retrieval due to the German embryo protection law. The benefit of prolonged culture is a better synchronization of the embryo and the uterine lining, as the state in which embryos after natural conception reach the uterus is that of a 4 or 5 day embryo. A blastocyst is a very good developed embryo on day 5.
Assisted Hatching
Hatching is made easier by thinning out the zona pellucida (the egg coat, the cell membrane around the egg) with a laser. In some cases this safe method can help the embryo to leave the zona (hatch) and facilitate implantation.
Fertility protection and preservation
By the following methods fertility can be preserved for a later point in time. Reasons for taking this measures can be malignant diseases like cancer e.g. or if the personal environment requires it (partnership, job, age). We can offer you the following methods:
- 1. Cryopreservation of fertilized eggs
For couples it is possible to have their oocytes fertilized now and then preserved for transfer in the future - 2. Cryopreservation (vitrification) of unfertilized mature oocytes
Women without a partner can have their oocytes retrieved (after hormonal stimulation) and frozen by the ultrarapid freezing method called vitrification. At a later point in time the oocytes can be warmed and fertilized. Then a frozen embryo transfer can be performed. - 3. Cryopreservation of sperm
Spermatozoa also can be cryopreserved. - 4. Cryopreservation of ovarian tissue
Ovarian tissue can be retrieved by laparoscopic surgery and frozen. The oocytes present in the ovarian cortex can be dissected later on, fertilized and transferred. This method is usually only performed in patients with cancer for fertility protection.